Is Creatine Safe for Your Kidneys? What the 2026 Evidence Says
Two new meta-analyses confirm creatine monohydrate does not impair kidney function despite a modest bump in serum creatinine. Here's what the totality of evidence says — and why the myth has been so hard to shake.
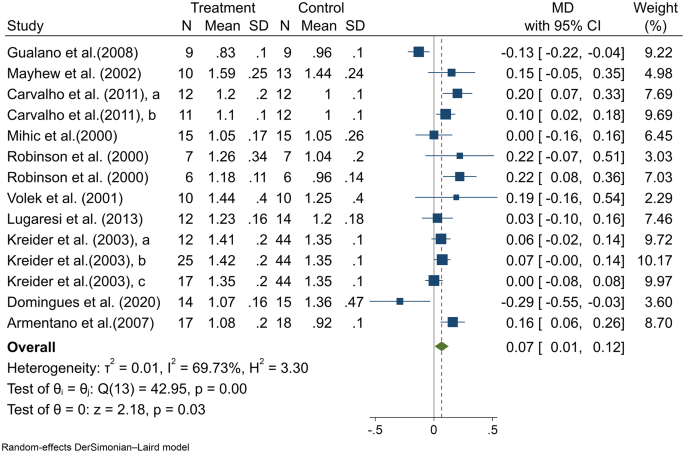
A 2025 systematic review with meta-analysis published in BMC Nephrology has delivered the most comprehensive answer yet to a question that has dogged the supplement for three decades: does it damage your kidneys? After pooling data from 12 randomized controlled trials — 177 people taking the compound, 263 on placebo — the answer is no. Serum creatinine does tick upward slightly, by a mean difference of 0.07 µmol/L, but that bump reflects normal metabolic breakdown rather than any meaningful deterioration in renal filtration. Glomerular filtration rate, the gold-standard measure of how well the organs are actually processing blood, showed no significant change.
To put that number in perspective: the average healthy adult’s serum creatinine sits somewhere between 60 and 110 µmol/L. A shift of 0.07 is a rounding error — clinically invisible, well within the noise of day-to-day biological fluctuation. And yet, because standard panels use this biomarker as their primary screening tool, people taking the powder have been flagged, worried, and sometimes told to stop — for decades.
Why this question won’t go away
The trouble starts with biochemistry. The compound, whether manufactured by your liver or swallowed as a powder, degrades into its metabolite at a steady rate. More of the precursor in circulation means more of the breakdown product in the bloodstream — regardless of what the filtering organs are doing. It’s a supply-side effect, not a filtration problem. Most GPs don’t routinely order cystatin C or a measured GFR; they run a basic metabolic panel, see elevated numbers, and the software raises a flag. That’s it. That’s the whole origin story of the kidney safety myth.
Elham Kabiri Naeini and colleagues at the University of Medical Sciences systematically searched the literature through mid-2025 and found 21 studies that met their inclusion criteria, 12 of which could be pooled for meta-analysis. The full review, published open-access in BMC Nephrology, examined serum creatinine, blood urea nitrogen, and estimated GFR — the three markers most likely to appear on a standard panel after someone starts supplementing.
“We found a small but statistically significant increase in serum creatinine,” the authors wrote, “likely due to metabolic turnover rather than renal impairment. No significant changes were observed in GFR, suggesting preserved kidney function.”
A separate 2026 meta-analysis of 19 randomized controlled trials, indexed on PubMed, came to the same conclusion. The metabolite rose — by roughly 0.13 mg/dL across pooled participants — but urea and eGFR stayed flat. Two independent research groups, two different search strategies, two different sets of inclusion criteria. Same answer.
The safety database is enormous
Even without the meta-analyses, the raw scale of the evidence should settle the question. Richard B. Kreider, a professor at Texas A&M who has studied this molecule for more than 25 years, led an international position statement published in Frontiers in Nutrition endorsed by more than 30 scholars worldwide. The group tallied over 680 peer-reviewed clinical investigations on the monohydrate form since the 1970s, involving more than 12,800 participants. Some protocols used intakes as high as 30 grams per day. Some ran for as long as 14 years.
The adverse-event picture from those 680-plus experiments is hard to argue with. Across the entire published record, 86.4% of investigations reported no side effects in the treatment arm beyond what the placebo group experienced. The compound was mentioned in just 0.00072% of 28.4 million adverse event reports spanning all FDA and EMA databases over five decades.
“Despite some anecdotal reports and experimental data suggesting that creatine could be deleterious to the kidneys,” wrote a group led by Bruno Gualano of the University of São Paulo in a 2023 narrative review in Nutrients, “cumulative evidence from independent, randomized controlled trials clearly show this is not the case.” Their paper, titled “Is It Time for a Requiem for Creatine Supplementation-Induced Kidney Failure?”, argued that the case reports linking the supplement to acute kidney injury were almost always confounded by dehydration, pre-existing disease, or contaminated products — not the molecule itself.
Once you’ve waded through the data, the question inverts. It’s not “is this safe for kidneys?” It’s “why did anyone ever think it wasn’t?”
The case reports that started it all
The scare traces back to a handful of case reports from the late 1990s and early 2000s — single patients, almost always young men, who presented with acute kidney injury and happened to be taking creatine. In nearly every instance, at least one major confound was present: extreme dehydration, concurrent use of nephrotoxic drugs, pre-existing renal pathology, or products adulterated with substances that were not what the label claimed.
Case reports can raise hypotheses. They can’t test them. The systematic reviews that came later tested them — and found nothing.
A short review of safety concerns published in Frontiers in Nutrition in 2025 walked through the most common fears — organ damage, dehydration, muscle cramping, gastrointestinal distress — and found that none of them stood up to the weight of randomized evidence. The dehydration anxiety, in particular, has been turned inside out: the supplement pulls water into muscle cells, and some research hints it may actually assist thermoregulation during exertion in hot conditions.
What about people with existing kidney disease?
Here the data gets thinner, and the responsible answer is “we don’t know enough to be confident.” Most participants in the meta-analyses were healthy adults with normal baseline function. A few small investigations have examined the compound in people with chronic kidney disease or type 2 diabetes, and they did not report worsening renal status — but the sample sizes were modest, the durations brief, and the designs often open-label.
A 2025 review in the Journal of Education, Health and Sport flagged this as the most conspicuous remaining gap in the literature. The authors concluded that the supplement appears safe for healthy organs but urged caution for anyone with diagnosed impairment. That’s not a warning about this particular substance — it’s the standard precaution that applies to any dietary product when you have an organ that isn’t working at full capacity.
If you have chronic kidney disease, the calculus shifts. Your renal clearance of the metabolite is slower to begin with, which means the conversion from precursor to breakdown product could amplify a signal that’s already outside normal range. No study has demonstrated harm in this population. But the absence of evidence isn’t evidence of absence when the trials simply haven’t been conducted at scale.
Why the myth is so hard to kill
Public belief about kidney damage from this supplement persists for reasons that extend well past the data. The lab-value confusion is genuinely tricky — it requires some biochemistry to grasp why a “high” reading can be physiologically normal. Kidneys are organs people are rightly protective of, and caution feels prudent even when it isn’t warranted by the studies. And the broader reputation of the dietary-supplement sector for adulterated goods and exaggerated marketing creates a guilt-by-association effect that clings to even the most thoroughly researched compounds.
Then there’s clinical inertia, which may be tougher to shift than any of the above. Medical school syllabi have been slow to update their teaching on sports nutrition, and a generation of physicians trained in the 1990s and 2000s absorbed the early case reports as fact. Reversing what a doctor learned in training demands decades of counter-evidence, and the literature on this topic — despite its volume — has not been packaged in a format that reaches the typical primary-care clinician. The Kreider position statement, with its 30-plus expert endorsements, represents an explicit attempt to bridge that chasm.
Creatine monohydrate is not some mystery powder. It is among the most researched supplements in existence, with a safety record that rivals common over-the-counter medications. The 2025-2026 body of evidence doesn’t just suggest it’s benign for renal function — it makes the case that the concern was never supported by anything stronger than a few unfortunate anecdotes that got amplified by a misunderstanding of basic biochemistry.
Practical takeaways
If you’re healthy and considering this supplement, the standard 5-gram daily dose of monohydrate is backed by decades of safety data. Tell your doctor you’re taking it — not because you need permission, but so they don’t misinterpret your next blood panel. If your creatinine comes back slightly elevated and your physician raises an eyebrow, you can point them to the Naeini et al. meta-analysis or ask whether they’d consider ordering a cystatin C test, which isn’t affected by creatine metabolism.
If you have kidney disease, the conversation with your nephrologist should happen before you start — not because the compound is known to be dangerous in this group, but because it hasn’t been studied enough to exclude risk.
The evidence has been accumulating for 30 years. The 2025-2026 systematic reviews are the capstone, not the foundation — they confirm what the broader research record had been saying all along. Creatine raises creatinine. It doesn’t harm kidneys. Those are different things.
Consult your doctor before starting any supplement, especially if you have pre-existing health conditions or are taking medications.
References
- Naeini EK, et al. Effect of creatine supplementation on kidney function: a systematic review and meta-analysis. BMC Nephrology. 2025. https://link.springer.com/article/10.1186/s12882-025-04558-6
- Kreider RB, et al. Creatine supplementation is safe, beneficial throughout the lifespan, and should not be restricted. Frontiers in Nutrition. 2025. https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2025.1578564/full
- Longobardi I, Gualano B, Seguro AC, Roschel H. Is it time for a requiem for creatine supplementation-induced kidney failure? A narrative review. Nutrients 15(6):1466. 2023. https://www.mdpi.com/2072-6643/15/6/1466
- Systematic review of creatine and kidney function in RCTs. PubMed. 2026. https://pubmed.ncbi.nlm.nih.gov/42035842/
- Short review of common safety concerns regarding creatine ingestion. Frontiers in Nutrition. 2025. https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2025.1682746/full
- Creatine supplementation and renal function — myths and evidence. Journal of Education, Health and Sport. 2025. https://apcz.umk.pl/JEHS/article/view/70576
The Vitalspell brief
Evidence-based supplement science — weekly in your inbox.
Subscribe

